


On Saturday March 30th 2019, a series of High Tea events will be held around the country by Endometriosis Australia to raise funds for endometriosis awareness, education and research. Share this by using #EndoMarch2019 on social media and visit www.endometriosisaustralia.org to purchase a ticket to your closest National EndoMarch High Tea.
Endometriosis Explained
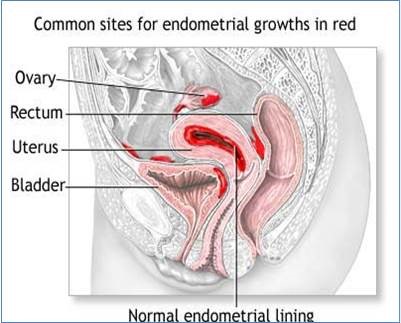
The endometrium is a thick lining of the uterus which is important for a healthy menstrual cycle and pregnancy. Endometriosis occurs when endometrial-like tissue starts to grow outside the uterus causing pain and potential infertility. This is the result of a chronic inflammatory reaction causing scar tissue formation and adhesions. As illustrated in the graphic below, the pelvis is the most common area of abnormal endometrial tissue deposition, but similar lesions may be seen at distant sites, such as the lung cavity, liver, kidneys, gluteal muscles, or bladder. It is estimated that 5-10% of women of reproductive age have endometriosis and the condition’s severity worsens with age.
Risk Factors
The most common risk factors are being single, delaying child birth or remaining childless, early menarche, the use of non-oral contraception, smoking, having a short menstrual cycle and longer duration of menstrual flow.
Signs and Symptoms
Pain and infertility are the most commonly occurring symptoms of endometriosis. Other symptoms include, dysmenorrhoea (painful periods), chronic pelvic pain, deep dyspareunia (painful sex), severe menstrual pain with irregular flow and premenstrual spotting. Some less common symptoms include dyschezia (painful defecation), hematochezia (rectal bleeding), dysuria (painful urination), and haematuria (blood in urine).
Treatment
Treatment is usually aimed at managing the symptoms of pain and infertility, but it also depends upon the age and fertility status of the woman. Management can be medical (involving drug therapy) or surgical, or a combination of both. Pain is often well managed with NSAIDs (e.g. Nurofen) with the surgical options of ablation of endometrial implants, resection of endometriomas or lysis of the adhesions. Other medical therapies which supress oestrogen (as increased oestrogen stimulates growth of endometriosis lesions) include oral contraceptive pills (eg Progestin), gonadotropin-releasing hormone (GnRH) agonists (eg Zoladex) and aromatase inhibitors (eg Armidex or Femara).
Infertility may be treated with surgery, ovulation induction or other assisted reproductive techniques. Although these treatments are potentially helpful, there is little evidence that the available treatment options significantly enhance fertility. Clinical trials are required to evaluate the efficacy of alternative treatment options.
AusTrials is conducting a phase 3 clinical trial to evaluate the efficacy and safety of a new medication, Relugolix ( 40 mg once daily) co-administered with low dose oestradiol and norethidrone acetate compared to placebo. The study will recruit premenopausal women aged 18 to 50 with the diagnosis of endometriosis confirmed by laparoscopy or laparotomy performed within the last 10 years, and have had 3 consecutive regular menstrual cycles.
For more information regarding this trial please contact us at AusTrials on 07 3278 5255 or by emailing info@austrials.com.au